
PUTTING A ‘DEFINITE’ FOOT FORWARD
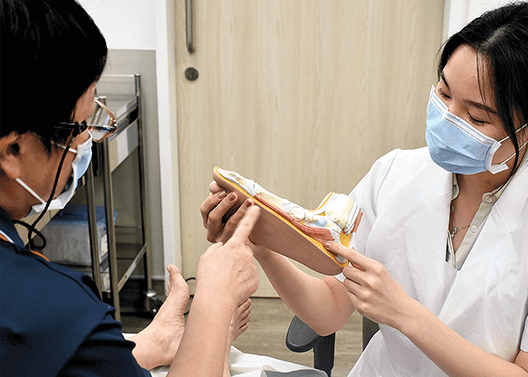
In June 2020, the Diabetic Foot in Primary and Tertiary (DEFINITE) Care programme was launched with funding from the Population Health Grant. DEFINITE Care is a first-of-its-kind programme that aims to coordinate multidisciplinary care across Primary and Tertiary clinical settings for patients with diabetic foot ulcers (DFU) to prevent diabetes-related lower limb amputations. This in turn lowers the disease burden of DFU within NHG and Singapore. Services for patients with DFU are integrated across National Healthcare Group Polyclinics (NHGP), Tan Tock Seng Hospital (TTSH), Khoo Teck Puat Hospital (KTPH), and the upcoming Woodlands Health (WH).
The DEFINITE Care team engaged more than 60 healthcare professionals from NHG Institutions to form a multidisciplinary DFU care team (comprising Vascular Surgery, Endocrinology, Orthopaedics Surgery, Primary Care, Podiatry, and Nursing). Under the programme, a new role, Diabetic Foot Coordinator (DFC), will ensure care integration, improved monitoring and patient adherence, and improved patient outcomes across primary and tertiary care. A DEFINITE Registry was established, in collaboration with NHG’s Health Services & Outcomes Research (HSOR) Department, which analysed the cost-effectiveness, cost-utility, and long-term sustainability of the programme. This would help facilitate the scale and spread of the model beyond NHG to other clusters. The DEFINITE Care programme partnered the Lee Kong Chian School of Medicine (LKCMedicine), Skin Research Institute of Singapore (SRIS), Agency for Science, Technology and Research (A*STAR), and industry collaborators to study the efficacy of a patient-centric wound care app. This enabled the tracking and monitoring of wounds, and early detection of deterioration by leveraging Artificial Intelligence (AI) and deep learning via wound image analysis, in order to prevent diabetes-related amputations.
Preliminary data has shown more than 2,800 patients benefitting from the programme to-date. Minor and major amputation rates have dropped, and diabetes and hyperlipidaemia control among DEFINITE patients has improved.

CONTINUING CARE WITH TELEHEALTH SERVICES
Yishun Health’s Population Health and Community Transformation (PHCT) team continued to help residents manage their chronic conditions by increasing the number of Community Nurse Post (CNP) sessions, leveraging technology and conducting teleconsultations. The service catered to two groups of resident patients: seniors with stable long-term conditions, and seniors with more complex issues who required closer medical supervision. The PHCT team also piloted a Telehealth Kit for residents who did not have digital devices. The kit consists of a tablet and health monitoring devices, such as automated blood pressure monitors, thermometers, and weighing scales. This allowed residents to consult nurses on their conditions remotely.
Between April and September 2020, PHCT reached 1,330 residents.

CARING FOR PATIENTS AT HOME
To continue caring for patients transiting from hospital to home and relieve the surging demand for hospital beds, the Yishun Health Ageing-In-Place Community Care Team (AIP-CCT) ramped up its capacity to care for more patients with medical needs at home. The AIP-CCT redesigned its service to include intensive and continuing home rehabilitation for Hip Fracture, Orthopaedic, Neurology, and General Medicine patients. From April to September 2020, there was a 21 per cent increase in patient enrolment, as well as a 30 per cent increase in home visits made by the team as compared to FY2019.
BUILDING PARTNERSHIPS

WH has been serving and engaging residents in Northern Singapore since 2016. During the Circuit Breaker in 2020, WH collaborated with community partners to stay connected with patients and monitor their health.
Partners included the Ministry of Social and Family Development (MSF), SATA CommHealth, the Asian Women’s Welfare Association (AWWA), Muis, MENDAKI, MESRA (M3), Masjid Yusof Ishak, and schools such as Christ Church Secondary School, Riverside Secondary School, as well as Republic Polytechnic and Nanyang Polytechnic.
Through these collaborations, WH reached out to more than 500 residents and 2,000 students virtually and through house visits in 2020. Residents who needed support were referred for follow-up at Community Nurse Posts (CNPs). SATA CommHealth’s Doctors-On-Wheels sessions were introduced to make primary care easily accessible to the neighbourhoods.

ANG MO KIO SPECIALIST CENTRE
Nestled in Central Zone, the Ang Mo Kio Specialist Centre (AMKSC), set up by TTSH in close collaboration with primary care and community partners, opened in December 2019. AMKSC provides holistic specialist care that includes:
- An eye clinic that accepts referrals from GPs for patients with stable chronic eye conditions.
- Additional diagnostic hearing tests for residents who have abnormal hearing results, following basic functional screening.
- Integrated musculoskeletal services where patients from polyclinics or GPs are triaged to consult occupational therapists/physiotherapists for timely treatment before their Specialist Outpatient Clinic (SOC) appointment.
- Trans-disciplinary care where clinical diabetes educators, as well as GPs, collaborate to support patients with Diabetes Mellitus (DM).
- Co-located integrated health and social care services.
AUGMENTING CARE AND EMPOWERING RESIDENTS
WH introduced several initiatives to augment care in the community and empower residents to take charge of their own health.
- The Urgent Care Centre (UCC) at Kampung Admiralty (UCC@Admiralty) is equipped to handle urgent and acute conditions, reducing the need for residents to visit the hospital emergency department. It has seen more than 4,000 patients between September 2020 and April 2021.
- In September 2020, WH launched its GPFirst Programme in the North to encourage residents to first seek care for non-emergency conditions from their family doctor. To-date, WH in partnership with Yishun Health has engaged 139 GPs in Woodlands, Sembawang and Yishun, and recruited 81 for the programme as of June 2021. Between September 2020 and February 2021, 1,205 GPFirst referrals were made to the UCC@Admiralty and KTPH’s A&E.
- In FY2020, WH Community Nurses provided care to more than 240 unique residents at the eight CNPs. Five CNPs have started to offer teleconsultation.
EQUIPPING COMMUNITY PARTNERS
The Assessment Shared Care Teams (ASCAT) is an adult community psychiatric programme which manages patients in the community with mild to moderate mental health conditions. The Institute of Mental Health (IMH) ASCAT team, comprising doctors, nurses, Medical Social Workers (MSWs), and case managers, trains and supports polyclinic doctors through co-consultations.
In FY2020, ASCAT hosted one training workshop and numerous case discussions with community partners. 88 per cent of the community partners reported they achieved an 80 per cent improvement in their understanding on mental health. 100 per cent of clients who were enrolled in the ASCAT programme reported an increase in their quality of life as compared with 63 per cent of clients in FY2019.
SUPPORTING SENIORS WITH MENTAL HEALTH ISSUES
In FY2020, the Aged Psychiatry Community Assessment and Treatment Service (APCATS) — a community-oriented psycho-geriatric outreach service that promotes ageing-in-place for seniors with mental health issues — conducted 75 first visits and 881 repeat visits to seniors who faced challenges accessing mental health services. This helped reduce caregiver burden and prevented unnecessary admissions, especially during the COVID-19 pandemic.
The team implemented virtual consultations with patients at home or in nursing homes. In addition, community partners were equipped with knowledge and skills in depression and dementia care.
HELPING PATIENTS TO REINTEGRATE INTO THE COMMUNITY
In 2015, IMH collaborated with the Agency for Integrated Care (AIC) and started the Aftercare Programme for one pilot site and one community partner to provide intensive case management and care planning for cases in the community with complex needs. In tandem with close monitoring, patients adhered more to treatment and sustained good mental health. As a result, readmission rates and emergency room visits declined. IMH also worked with community partners to ensure patients stayed on track to recovery.
As of March 2021, IMH collaborated with five community partners and enrolled 1,842 patients in the programme, as compared to 1,540 patients in FY2019.
INTEGRATING MENTAL HEALTH INTO PRIMARY CARE

INTEGRATING MENTAL HEALTH INTO PRIMARY CARE
On World Mental Health Day in October 2020, NHGP partnered the Women’s Executive Committee of Nee Soon East Community Club and the People’s Association (PA) Women’s Integration Network (WIN) Council to conduct a talk, Manage Your Mind & Fight the Fear. It discussed management of individual mental health and anxiety.
NHGP also worked with TOUCH Community Services (TCS) between October and December 2020 to organise a series of talks, The 2 Challenges in Senior Years — Dementia and Depression. Conducted in English, Mandarin, and Malay, the session covered how to enhance quality of life and age healthily in the community in spite of these two conditions.

IMPROVING AWARENESS ON MAMMOGRAM SCREENING
In November 2020, National Healthcare Group Diagnostics (NHGD) created a “three-bead keychain” as a visual tool to educate and promote the importance of early detection of breast cancer through mammogram screening. NHGD also implemented a new self-service appointment system that improved community access to mammograms. The new E-bookings increased by 70 per cent within the first month of the launch.