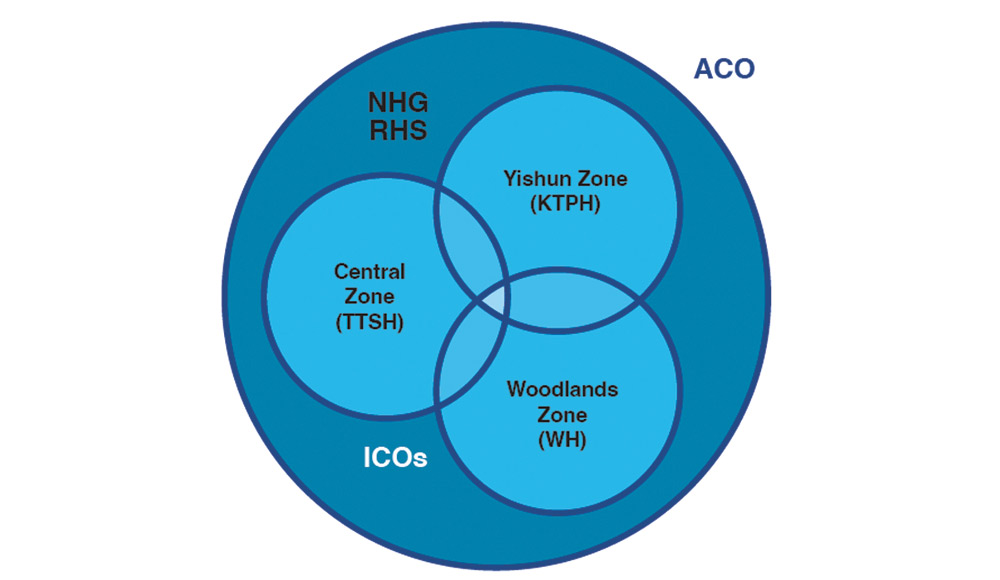
 Figure 1: NHG’s ACO-ICO Model
Figure 1: NHG’s ACO-ICO Model
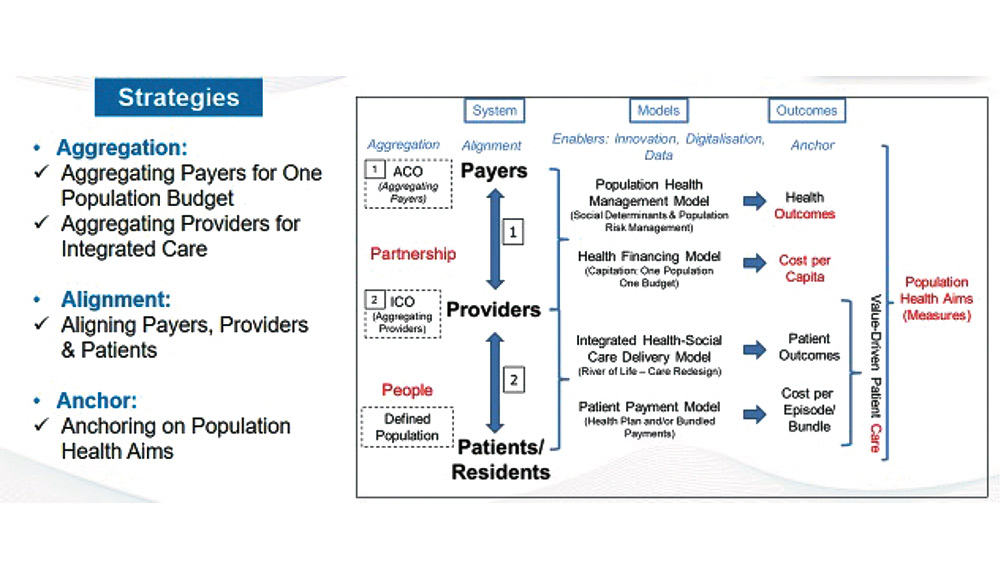 Figure 2: ‘Triple A’ Strategy for Population Health Aims
Figure 2: ‘Triple A’ Strategy for Population Health Aims
INTRODUCING NHG’S ACO–ICO MODEL
To better address the needs of an ageing population, manage rising chronic disease burden, and bridge the gap between the health and social needs of Singapore residents, NHG has redesigned its healthcare delivery system to move from managing patients, to supporting residents in their health journey.
To drive a sustainable healthcare ecosystem, NHG re-organised itself to align with an Accountable Care Organisation (ACO)–Integrated Care Organisation (ICO) model in 2021. As an ACO, NHG is responsible for the health outcomes, care, and costs of 1.5 million Singapore residents living in the Central-North region. To enable locality-based planning and care provision, our zones — Central Health (CH), Yishun Health (YH), and Woodlands Health (WH) — are designated as ICOs. The ICOs are supported by NHG Polyclinics, the Institute of Mental Health (IMH), and the National Skin Centre (NSC). Each ICO serves the care needs of its zonal population through a strong network of like-minded partner providers to deliver joined-up, value-based, and person-centred care (see Figure 1).
NHG’s ACO-ICO model Aligns, Aggregates and Anchors all actors in the system, namely the payer, provider, and patient/resident. This ‘triple A’ strategy incentivises the behaviours of all actors towards health, reduces fragmentation, and provides stackable value across the system, driving towards our Population Health Aims (see Figure 2).

DRIVING CARE TRANSFORMATION FOR POPULATION HEALTH
In tandem with the Ministry of Health (MOH)’s Healthier SG initiative, NHG has kick-started its efforts in (i) Building Relationship-Based Care and (ii) Strengthening Place-Based and Integrated Care.
Building Relationship-Based Care
NHG is gradually shifting from episodic transactional provider-patient exchanges to a longitudinal care relationship between the resident and his/her primary care provider via enrolment to a dedicated primary care provider such as a Family Physician or General Practitioner (GP). This empowers the resident to own his or her health. The primary care provider would then co-create a care plan with the resident that would strongly feature preventive health elements. This close relationship with a primary care provider is expected to enable each resident to better understand his or her health profile with periodic reviews, set personalised care goals, and navigate the co-created care plan.
Strengthening Place-Based and Integrated Care
The resident and the GP are supported through a Place-Based Care approach that comprises partnerships with health and social care partners, within a geographical-based Community of Care (CoC). The CoC supports the health and social care needs of the local residents. It ensures that care is localised to the needs of residents at a neighbourhood level, and that there is an availability of programmes offered by local health and social care partners. As of July 2022, NHG, with support from the three ICOs, has set up 41 CoCs. Expansions are on-going to build a CoC in every neighbourhood for our residents.
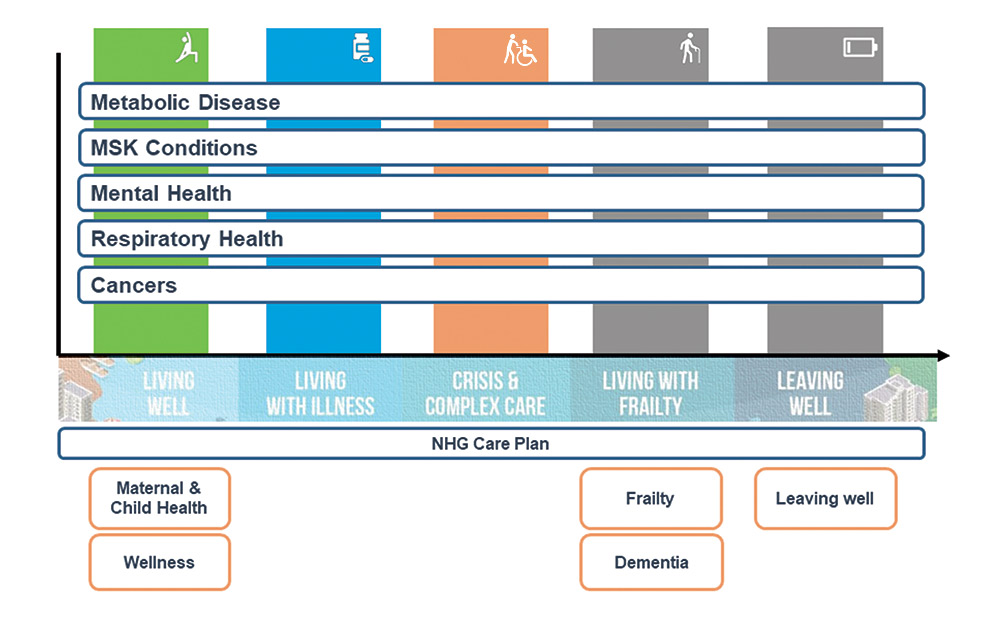
Integrated Care adopts a life-journey approach that involves the design of programmes and pathways that joins up and simplifies care for residents across their preventive, pre-disease, and end-of-life needs. The keystone of integrated care will be GPs, being the first and constant point-of-contact in the residents’ health journey. CoCs within each region support GPs to help each resident access programmes and services in the community, near their homes to help them attain their health goals. Underpinning the integrated care plans is the NHG strategic clinical priorities driven by the population level burden of disease projections, namely, for Metabolic Disease, Musculoskeletal, Chronic Respiratory and Mental Health conditions, and Cancers. For the effective management of these conditions, NHG established a framework that is supported by a multidisciplinary care team provided by an ICO that serves the local care needs of residents. This would enable NHG to drive integrated population health across the Central-North region, align interests, financing, and workflows between care providers, and anchor care in the community.
KEY ENABLERS TO DRIVE CARE TRANSFORMATION
Capitation Financing
Singapore’s Healthier SG initiative has paved the way for the three public healthcare clusters to move away from a workload-based funding model towards capitation (per-resident) funding. Singaporeans and Permanent Residents will be assigned to a healthcare cluster based on their geographical residence. Each cluster will be responsible for its assigned residents’ health experience, outcomes, and costs. As an ACO, NHG will optimise the capitation funding for residents in the Central-North region, through more holistic end-to-end care executed jointly with its Institutions, care provider partners, and other government agencies.
The Group Accountable Care (GAC) Office within NHG will allocate the resources to its providers to incentivise population health efforts, behaviours and outcomes, and for joined-up care to be put in place for residents.
Data Transformation
The GAC Office is building a Population Health Registry (PHR) that will include resident-data, in addition to patient-data, to create a longitudinal record of the health, social, and lifestyle factors of all residents who live within the Central-North region, including patients of NHG Institutions. When fully operational, NHG will be able to segment the population based on risk factors, identify high-risk individuals for intervention, perform geospatial analyses to identify geographical areas where residents have specific healthcare needs, and assess the impact and effectiveness of implemented interventions. The past year has seen the PHR team focused on creating a longitudinal database using NHG institutional data to cater for a cross-institution analysis for each ICO to analyse the profile of each of their assigned resident population. Moving forward, data from non-NHG sources, including our GP and community partners, will be included. Dashboards are in the pipeline to allow for the monitoring of resident population health outcomes at different levels.

 The launch of Population Health Collective by Health Minister Ong Ye Kung.
The launch of Population Health Collective by Health Minister Ong Ye Kung.
LAUNCH OF POPULATION HEALTH COLLECTIVE
In May 2022, Minister for Health Mr Ong Ye Kung launched NHG’s Population Health Collective (POPCollect) at the inaugural annual Population Health Connect (POPConnect) seminar. Hosted by NHG, POPCollect — comprising a network of more than 80 community partners, 544 GPs, agencies, and NHG Institutions — is a movement to improve the health and well-being of the population in Central-North Singapore through building a Community of Care (CoC) in every neighbourhood. POPCollect will form the basis for an annual workplan seminar to co-learn from one another and co-create meaningful collaborations for place-based care and relationship-based care.
