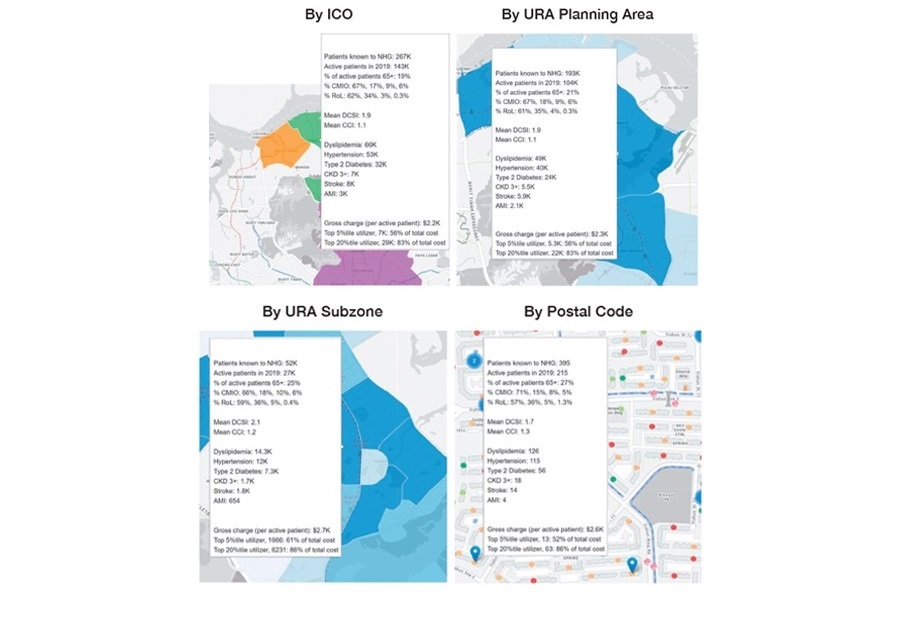
 Figure 1. Pop-up summaries of health information using the ICO planning dashboard
Figure 1. Pop-up summaries of health information using the ICO planning dashboard
Health Services and Outcomes Research (HSOR) supports this care transformation journey by providing best available evidence for decision-making and knowledge translation to our stakeholders, and by building capacity and advancing knowledge in health services research.
DEVELOPING A DASHBOARD TO STUDY THE NHG POPULATION
HSOR collaborated with Group Integrated Care (GIC) to develop a planning dashboard that provides stakeholders with a platform to explore aggregated demographic and healthcare data on patients residing in the NHG catchment area. Viewed through a system comprising maps, charts, and tables, users are able to examine data on demographics, chronic disease prevalence, ROL segments of care, and healthcare utilisation, as well as overall and per capita healthcare cost of known patients. Additionally, the dashboard includes information on the Community Health Assist Scheme General Practitioner (CHAS GP) clinics within the Central-North region, and clinic-level data. The data is presented via four geographic segmentations: i) Integrated Care Office (ICO), ii) Urban Redevelopment Authority (URA) planning area, iii) URA subzone, and iv) postal code (Figure 1). Available are summarised data sets of specific locations. This comprehensive overview of the NHG patient population will help stakeholders gain a deeper understanding of our patients, to better inform and facilitate resource and policy planning.
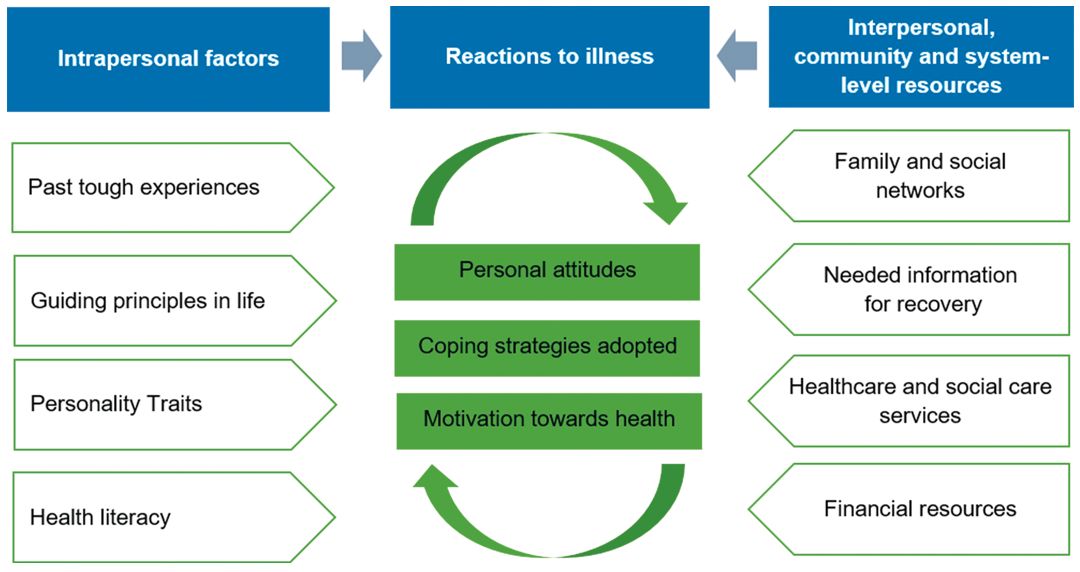 Figure 2. Factors influencing health resilience and their processes and interactions.
Figure 2. Factors influencing health resilience and their processes and interactions.
IDENTIFYING FACTORS ASSOCIATED WITH RESILIENCE IN THE COMMUNITY
Some 65 residents living within the Central-North region of Singapore were interviewed in a qualitative study, to understand their perspectives on how they prepared for, dealt with, and overcame challenges and the impact of health adversities. These residents had experiences of being unwell, or taking care of someone who had been unwell in the past 5 years, and were from varying age groups. Semi-structured interviews were conducted with the participants, of which 14 were caregivers. Health resilience was found to be dynamic and comprised systemically impacted multi-layer interactions across interlinked, intrapersonal, reaction-related, interpersonal, community, and system-level factors (Figure 2). Intrapersonal factors, such as previous tough life experiences, guiding principles in life, personality traits, and health literacy, were interlinked closely with perceived availability, accessibility or support accorded by community and system-level resources. These intra-, inter- and extra-personal factors influenced one’s reactions to illness, such as personal attitudes, coping mechanisms adopted, and motivation towards health, which ultimately influenced the individual’s ability to manage external and internal demands of their health challenges. Identifying the factors that influence health resilience and understanding their processes and interactions can help inform public health services on how to better support individuals to minimise or overcome the ill effects of health and life adversities.
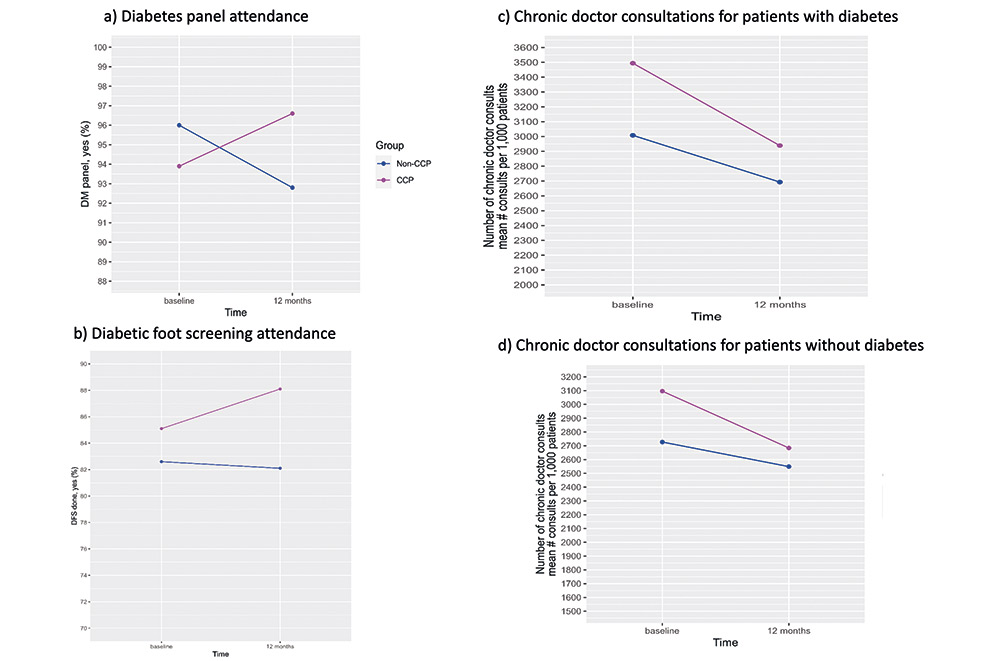 Figure 3. Adherence to care processes and chronic doctor consultations
Figure 3. Adherence to care processes and chronic doctor consultations
EVALUATION OF A CHRONIC CARE PLAN AT ANG MO KIO POLYCLINIC
The Chronic Care Plan (CCP), a pre-paid bundle payment scheme, was introduced at Ang Mo Kio Polyclinic in January 2019. Key features included (i) pre-payment using Medisave and Flexi-Medisave and/or out-of-pocket, (ii) enrolment incentives, (iii) shared decision-making on chronic disease management, and (iv) financial rewards for achieving pre-specified health targets. A study was conducted to evaluate the impact of CCP on patients’ adherence to care processes, chronic disease control, polyclinic healthcare utilisation, and total polyclinic gross charges at 1 year. Patients who had similar characteristics to the CCP patients and were followed up at the polyclinic for chronic conditions, but not enrolled in CCP, served as the control group.
At 1 year, CCP patients with diabetes (n=2,359) were more likely to adhere to the diabetes test panel and foot screening compared to the control group, and a larger decrease in the number of doctor consultations for chronic care was observed. A similar decrease was also noted in the 2,455 CCP patients without diabetes (Figure 3). No significant differences were observed in chronic disease control, polyclinic healthcare utilisation, and total polyclinic gross charges. Findings suggest that a pre-paid chronic care financial package coupled with financial incentives could be useful to encourage adherence to care processes.